What an anterior pelvic tilt is, what it means for you, and how you can fix it
Body Mechanics

Understanding the anteroposterior pelvic tilt (APT)
Understanding the anteroposterior pelvic tilt (APT) Anterior pelvic tilt isn't just a posture issue—it’s a functional limitation that disrupts load transfer, breathing mechanics, and core stability. In a healthy body, the pelvis should move freely between anterior and posterior tilt to accommodate different positions and loading demands (e.g., squatting, walking, jumping). When this dynamic movement is lost and the pelvis becomes chronically anteriorly tilted, the surrounding musculature adapts in dysfunctional ways that reinforce the misalignment. This leads to compensatory pain and compression in the lower back, which disrupts performance and diminishes daily quality of life. | 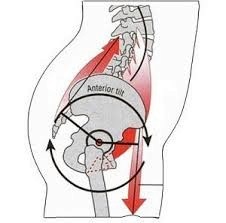 |
How to think about the pelvis
The pelvis is like a bowl filled with water. When the pelvis is in a neutral position, the bowl stays level and no water spills out. However, when the muscles surrounding the pelvis become overactive or shortened, they pull the pelvis in different directions, causing the “water to spill” and leading to postural compensations.
Posterior pelvic tiltA posterior tilt occurs when the back of the pelvis tips downward, causing the “water” to spill out the back. When this happens, the hamstrings and core co-contract—The hamstrings pull the back of the pelvis down, while the core pulls the front of the pelvis upward. | Anterior Tilt 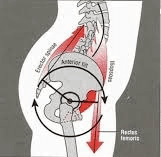 |
Anterior pelvic tiltAn anterior pelvic tilt occurs when the back of the pelvis is pulled upward and the front is pulled downward. In this case, the lower back and rectus femoris co-contract—The lower back lifts the back of the pelvis, while the rectus femoris pulls the front downward. | Posterior Tilt 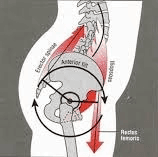 |
In a neutral posture
With a neutral pelvic posture—or, more importantly, a hip with adequate, controlled mobility—you can transition cleanly between these positions depending on the task.
For example, during hip flexion, the pelvis should tilt anteriorly. As you return into hip extension, the hamstrings must have the strength to pull the pelvis posteriorly, returning it to a neutral position.
What's happening in the body
APT is caused by a combination of overactive, shortened muscles and underactive, lengthened ones.
Muscles That Become Overactive or Shortened:
Hip Flexors (especially iliacus and rectus femoris) are chronically shortened and pull the pelvis downward at the front.
Spinal Erectors (e.g., lumbar paraspinals): Extend the lumbar spine, reinforcing the arch. In the lower back
TFL: assists with hip flexion and contributes to compensation, especially if the glutes are offline. (ask the couch for more information)
Muscles That Become Inhibited or Lengthened:
Glute Max and Med: lose mechanical advantage and fail to pull the pelvis posteriorly.
Hamstrings (medial group): lose their posterior tilt function at the hip.
Deep Core (transverse abdominis, internal obliques): becomes weak, losing tension between the ribcage and pelvis.
Adductors: often weak or inactive, further reducing internal stabilization of the pelvis.
The consequences
The pelvis becomes locked in a forward-tilted position. This can result in:
Compressed lower back
Rib flare and poor intra-abdominal pressure
Overuse of quads, hip flexors, and lumbar spine in basic movement tasks
Reduced posterior chain engagement in walking, lifting, squatting, etc.
How to Fix It: Restoring Pelvic Neutrality and Control
To restore optimal pelvic control, we need to retrain both mobility and stability. The goal is not to “tuck the pelvis” into posterior tilt permanently, but to restore access to full pelvic range and teach the body how to use it under load.
Inhibit Overactive Muscles
Use soft tissue release and lengthening techniques for:
Rectus femoris and iliacus (front of the hip): Rectus Femoris Myofascial Release, Couch Stretch
Spinal erectors (low back): Jefferson Curl
TFL if it’s assisting with flexion and pelvic tilt: Terminal Lift-off TFL Stretch
Ltisimis dorsi, which pulls the pelvis into an anterior tilt when arms come overhead: Lat Myofascial Release
Re-activate Inhibited Muscles
You’re not just trying to “strengthen the glutes”—you’re re-training neuromuscular timing so the right muscles fire in the right order:
Hamstrings + Abs Co-Contraction: Adducted Harop Curl, 90-90 hamstring core co-contraction
Glute Max Activation: Adducted SL RDL
Adductor/Anterior Pelvic Floor Obliques and TVA: Adducted Floor Bridge - Cross Body Tap
Integrate into the movement
Maintain neutral pelvis during shoulder flexion: Tall Kneeling Press to Y Raise
Maintain rib cage pelvic co-contraction during hip extension; Adducted Harop Curl, Sissy squat, Zercher ATG Split Squat.
Maintain a neutral pelvis during hip flexion. Heel-Elevated Zercher Squat.
Final Thought
Anterior pelvic tilt is not the enemy—but being stuck in it is. The real goal is to regain dynamic control of the pelvis across positions, which unlocks strength, reduces compensation, and prevents chronic overload to structures like the low back, quads, and hip flexors.

Training Strategies
The Role of Stretching: What it Does and Doesn’t Do
Stretching is often treated as a warm-up formality or a cool-down ritual—with little attention paid to the neurological and biomechanical nuances that distinguish one method from another. Stretching isn’t a one-size-fits-all practice. It’s a tool. And the way it’s applied should depend on the outcome you’re targeting—whether that’s joint integrity, end-range control, fascial tensioning, or recovery.

Body Mechanics
What is scapular winging, and how do we treat it?
Scapular winging occurs when the medial (inner edge) and inferior (bottom corner) aspects of the scapula (shoulder blade) lift away from the rib cage. This often becomes visible during scapular depression and retraction (pulling the shoulder blade down and towards the spine), but in many cases can also be seen at rest.

Body Mechanics
What is scapulo-humoral rhythm, and why does it matter
Scapulohumeral rhythm describes the coordinated movement between the shoulder blade (scapula) and the upper arm bone (humerus) during arm elevation, such as abduction. After the first ~30 degrees of humeral abduction (think of the early part of a lateral raise), the scapula begins to upwardly rotate in a consistent 2:1 ratio with the humerus — for every 2 degrees the humerus moves, the scapula rotates 1 degree.