What is scapulo-humoral rhythm, and why does it matter
Body Mechanics

About
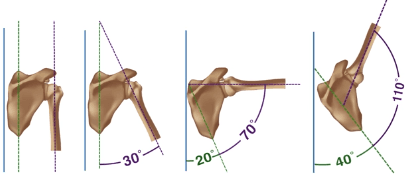
Scapulohumeral rhythm describes the coordinated movement between the shoulder blade (scapula) and the upper arm bone (humerus) during arm elevation, such as abduction. After the first ~30 degrees of humeral abduction (think of the early part of a lateral raise), the scapula begins to upwardly rotate in a consistent 2:1 ratio with the humerus — for every 2 degrees the humerus moves, the scapula rotates 1 degree.
The function
This synchronized action maintains optimal alignment between the humeral head and the glenoid cavity, ensuring smooth movement, efficient force production, and proper shoulder mechanics. Without it, the scapula and humerus would move out of sync, increasing the risk of impingement, instability, and shoulder injury.
Muscles involved
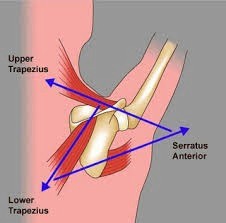
The primary muscles responsible for upward rotation of the scapula are the serratus anterior and the lower trapezius. Together, they form the main upward rotation force couple:
|  | |
Additional contributors include:
We correct this misalignment and neuromuscular imbalance through a three-step process:
Middle trapezius – Acts as a stabilizer to control unwanted protraction and maintain smooth scapular tracking.
Rhomboids – Primarily downward rotators, but they provide stabilizing tension that prevents excessive scapular movement during arm elevation.
Rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis) – Not scapular movers, but critical for centring the humeral head in the glenoid, preventing impingement as the scapula rotates.
Why this matters
These muscles work together to keep the scapula and humerus in precise alignment, preventing crowding in the subacromial space and allowing powerful, pain-free overhead movement. Any weakness, tightness, or poor timing in this system can disrupt scapulohumeral rhythm, leading to decreased performance and higher injury risk.
When certain muscles become overactive or shortened, they can inhibit their counterparts through reciprocal inhibition. This prevents balanced activation, disrupts coordination between the scapula and humerus, and forces the body into compensatory movement patterns. Over time, these malalignments reduce posture quality, limit range of motion, and increase the likelihood of chronic pain or acute injury — especially in athletes who rely on repeated overhead actions.

Training Strategies
The Role of Stretching: What it Does and Doesn’t Do
Stretching is often treated as a warm-up formality or a cool-down ritual—with little attention paid to the neurological and biomechanical nuances that distinguish one method from another. Stretching isn’t a one-size-fits-all practice. It’s a tool. And the way it’s applied should depend on the outcome you’re targeting—whether that’s joint integrity, end-range control, fascial tensioning, or recovery.

Body Mechanics
What is scapular winging, and how do we treat it?
Scapular winging occurs when the medial (inner edge) and inferior (bottom corner) aspects of the scapula (shoulder blade) lift away from the rib cage. This often becomes visible during scapular depression and retraction (pulling the shoulder blade down and towards the spine), but in many cases can also be seen at rest.

Body Mechanics
When Synergists Take Over: Primary vs. Compensatory Pelvic Stabilizers (TFL + QL Dominance)
The primary stabilizers of the Lumbopelvic-Hip Complex (LPHC)—namely the glute max, glute med, medial hamstrings (semimembranosus/semitendinosus), transverse abdominis, and obliques—are responsible for centring the pelvis, controlling rotation, and maintaining neutral spine during movement. When these become underactive or neurologically inhibited, the body will seek secondary stabilizers to maintain functional movement, albeit at a cost to efficiency and joint health.