When Synergists Take Over: Primary vs. Compensatory Pelvic Stabilizers (TFL + QL Dominance)
Body Mechanics

Background
The primary stabilizers of the Lumbopelvic-Hip Complex (LPHC)—namely the glute max, glute med, medial hamstrings (semimembranosus/semitendinosus), transverse abdominis, and obliques—are responsible for centring the pelvis, controlling rotation, and maintaining neutral spine during movement. When these become underactive or neurologically inhibited, the body will seek secondary stabilizers to maintain functional movement, albeit at a cost to efficiency and joint health.
Synergistic Compensation by the TFL and QL
TFL (Tensor Fasciae Latae) CompensationFunction: The TFL is a hip flexor and weak internal rotator/abductor that’s technically part of the lateral chain but often overrecruits when the glute medius is offline. When the glute med or posterior glute fibres are inhibited:
| 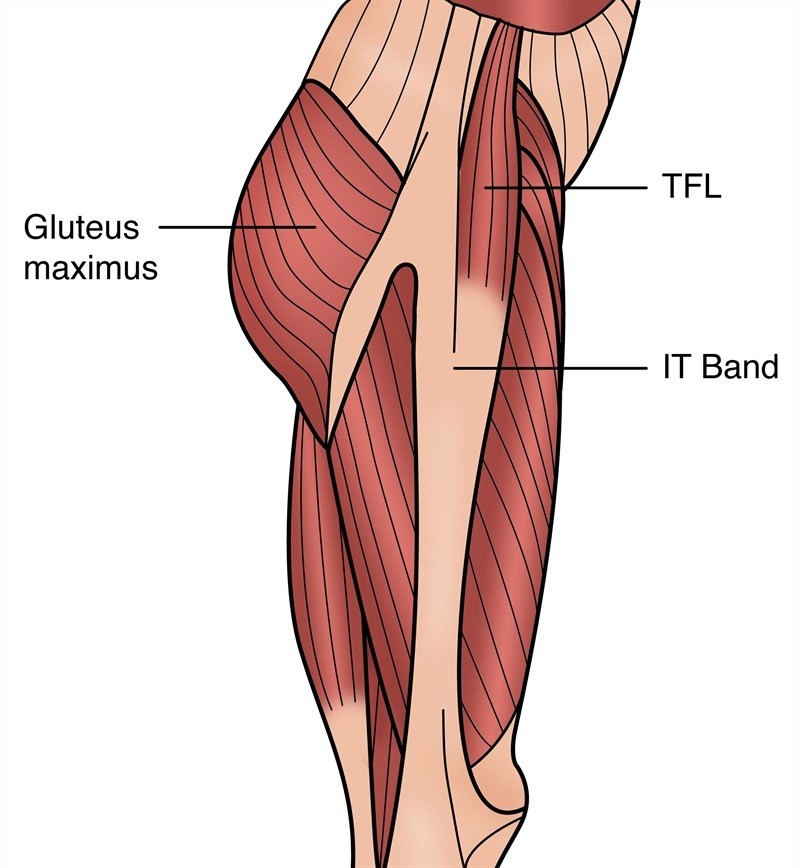 |
However, the TFL lacks the strength and lever arm of the glute med for accurate pelvic control, so this substitution leads to faulty motor patterning, especially excessive internal rotation and hip flexion during load-bearing tasks. This includes something as simple as walking, where poor glute med activation during midstance causes the hip to collapse outward into adduction. As the foot strikes the ground and the body transitions over it, the pelvis tilts and rotates inefficiently, and the TFL attempts to stabilize the hip from the front and side.
But because the TFL is oriented more anteriorly and doesn't provide true lateral support, it pulls the femur into further internal rotation and flexion instead of resisting collapse. The result is a chain reaction of misalignment: the knee dives inward, the arch flattens, and pelvic stability is compromised. Over time, this leads to chronic tension and overuse of the TFL, IT band stiffness, and often anterior hip pain during walking or standing.
QL (Quadratus Lumborum) CompensationFunction: The QL stabilizes the pelvis and assists with lateral spine flexion. When the medial hamstrings, core stabilizers, and glutes aren’t anchoring the pelvis: The QL "grabs" to control lateral sway. It compensates for a lack of deep abdominal wall control by stiffening the lumbar spine. During gait or hip flexion, the QL can drive asymmetrical pelvic positioning (e.g., hiking the left side to mimic single-leg stance stability). | 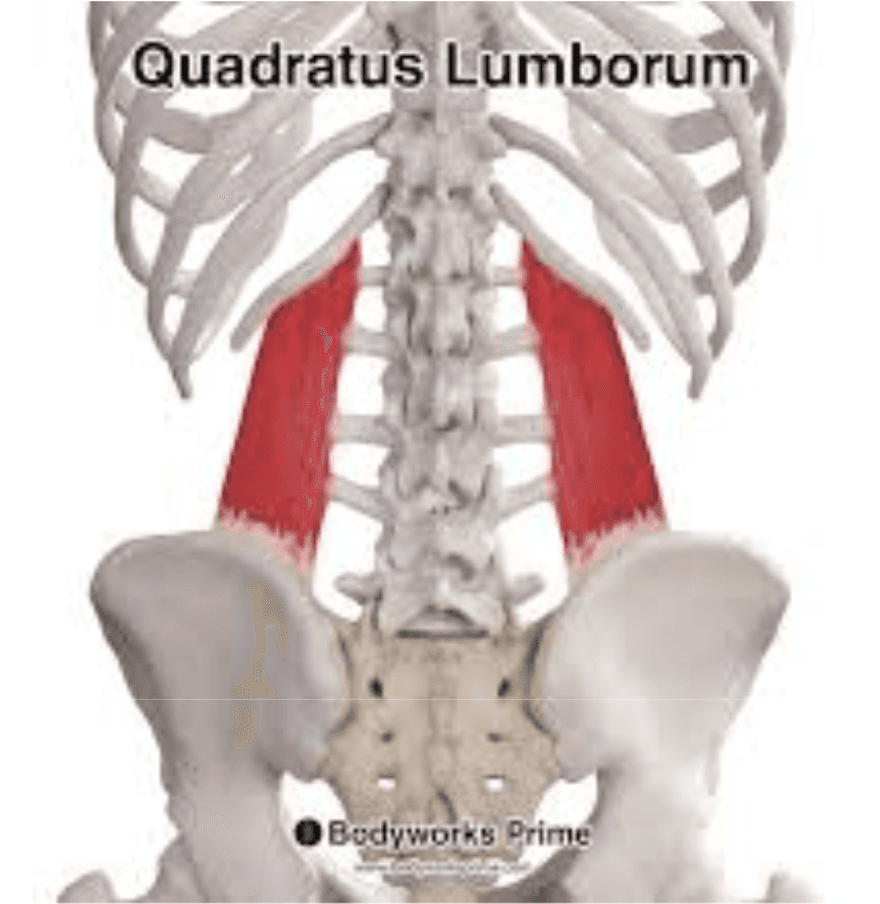 |
However, this strategy results in lateral compression of the lumbar spine and reduced spinal segmentation. It often co-occurs with contralateral oblique inhibition, meaning rotational control is also lost.
How They Work Together (Synergistic Compensation)
When primary stabilizers are downregulated, the TFL and QL become hyper-reliant teammates:
The TFL stabilizes the hip from below by gripping through the lateral line.
The QL stabilizes the pelvis and spine from above, compressing the rib cage downward toward the ilium.
This creates a closed, braced system that appears stable, but is actually rigid, asymmetrical, and prone to overuse injuries.
How to Combat This
Correcting synergistic dominance and restoring LPHC stability begins with reactivating inhibited primary stabilizers and reducing compensation patterns through targeted neuromuscular retraining. The approach should be phased, addressing mobility, activation, and integration:
Inhibit Overactive Synergists
Begin with myofascial release and stretching for the TFL and QL to reduce their hypertonicity and allow space for proper muscle recruitment patterns to emerge.
TFL: Use foam rolling or a lacrosse ball just below the ASIS and lateral hip. Follow with kneeling hip flexor/abductor stretches.
QL: Apply pressure along the lower back and posterior ribs, and use side-lying or wall-assisted lateral stretches.
Activate Primary Stabilizers
Restore function to the glutes, medial hamstrings, and deep core through isolated activation drills and targeted patterning.
Glute Medius: Clamshell Star Plank, SL Box Hinge - Cross Body Reach
Glute Max: Floor bridge,
Deep core: Diaphragmatic Breathing
Integrated applied movement
As awareness improves, build in controlled, integrated patterns that train practical hip function with a focus on anti-rotation and unilateral work.
Glute Medius: Adducted SL RDL, Weighted Hip Airplane
Glute Max: SL Slider Step Down, SL Step Down
Deep Core: Adducted Floor Bridge - Cross Body Tap, Adducted Reverse Squat
Reinforce correct hip hinge and gait mechanics under controlled load and tempo.
Conclusion
If your glutes and deep core aren’t anchoring the pelvis, your body still has to create stability—so it borrows it from the TFL and QL. That strategy works short-term, but it’s rigid and inefficient: the hip loses clean control, the knee and foot start compensating, and the low back often becomes the “stability engine.” The solution isn’t more bracing or more stretching—it’s restoring the right hierarchy: downshift the synergists, reactivate the primary stabilizers, then reintegrate that control into real movement like hinging, gait, and single-leg loading.
If you want, paste your exact draft and I’ll do a true blog edit (same ideas, same voice) with clean headings, skimmable sections, and a tighter flow.

Training Strategies
The Role of Stretching: What it Does and Doesn’t Do
Stretching is often treated as a warm-up formality or a cool-down ritual—with little attention paid to the neurological and biomechanical nuances that distinguish one method from another. Stretching isn’t a one-size-fits-all practice. It’s a tool. And the way it’s applied should depend on the outcome you’re targeting—whether that’s joint integrity, end-range control, fascial tensioning, or recovery.

Body Mechanics
What is scapular winging, and how do we treat it?
Scapular winging occurs when the medial (inner edge) and inferior (bottom corner) aspects of the scapula (shoulder blade) lift away from the rib cage. This often becomes visible during scapular depression and retraction (pulling the shoulder blade down and towards the spine), but in many cases can also be seen at rest.

Body Mechanics
What is scapulo-humoral rhythm, and why does it matter
Scapulohumeral rhythm describes the coordinated movement between the shoulder blade (scapula) and the upper arm bone (humerus) during arm elevation, such as abduction. After the first ~30 degrees of humeral abduction (think of the early part of a lateral raise), the scapula begins to upwardly rotate in a consistent 2:1 ratio with the humerus — for every 2 degrees the humerus moves, the scapula rotates 1 degree.